“Health matters. But the bigger goal is raising a child who can thrive, live with others, and grow into a good person.”
What does it mean to raise a good child — not just a healthy one?
That single question governs every section of this guide. Modern parenting culture has been shaped by medicine, therapy, and social media — and each of those forces tends to narrow the lens. The doctor focuses on physical health. The therapist focuses on emotional safety. Online advice often rewards what is vivid, emotionally charged, or highly shareable. But none of them alone captures what parents in every generation have really been reaching for: a child who is healthy and good, emotionally capable and morally formed, independent and caring toward others.
This WYSK insists: health matters — but the bigger goal is raising a child who can thrive, live with others, and grow into a good person.
What You Should Know — and Why You Should Care
You are raising a child in a world that is louder, faster, and more digitally saturated than many parents expected. The same phone that shows you a breastfeeding support group at midnight also shows you a stranger calling a nursing mother “disgusting.” The same internet that offers evidence-based child development research also serves you a viral claim that screen time “causes autism.”
This guide covers ten issues that touch almost every family with a child between birth and age five. For each one, you will find honest answers to three questions: What do most people believe? What does the best evidence actually say? And what matters most long-term — not just medically, but as a matter of character and values?
Clear moral teaching and warm parenting are not rivals. Respect without firmness can become indulgence; firmness without respect can become fear. The goal is both.
You don’t need to be perfect. But you do need to be intentional — because children learn values from what we tolerate, not just what we say.
Critical Issues (Table of Contents)
I. Breastfeeding Beyond Infancy
II. Values and Character Formation
III. Big Feelings: Tantrums, Meltdowns, and Emotional Regulation
IV. Discipline and Consequences: Authority Without Cruelty
V. Sleep: The Invisible Driver
VI. Bottles, Food, Picky Eating, and Control
VII. Pacifiers and Thumb-Sucking
VIII. Screens and the Digital Ecosystem
IX. Developmental Milestones: “Is My Child on Track?”
X. Toilet Training, Bodily Autonomy, and Shame
Reliable Resources (separate required section)
I. Breastfeeding Beyond Infancy
The Parent Worry
Parents — especially new mothers — carry enormous anxiety about feeding. Some fear they can’t produce enough milk. Others experience significant pain and feel shame about stopping. Many who breastfeed past a year face family pressure, side-eye from strangers, and cultural discomfort. And some mothers who stopped early feel guilt they don’t deserve. Structural realities — work schedules, lack of paid leave, access to lactation support, and infant care arrangements — shape what is practically possible for many families, independent of what they want or value.
What’s Normal at This Age
By 12 months, a baby eats solid foods alongside breast milk or formula. After 12 months, neither breast milk nor formula is the sole nutritional source. Breastfeeding after age one is common worldwide and is practiced by the majority of mothers in many countries; in the United States, rates of extended breastfeeding remain lower than international averages but have increased over recent decades.
What Mainstream Pediatric Guidance Emphasizes
The American Academy of Pediatrics (AAP) recommends exclusive breastfeeding for the first six months, followed by continued breastfeeding with complementary foods for at least two years and beyond — as long as it is mutually desired by mother and child.¹ The World Health Organization agrees. Breast milk continues to provide immunological benefits well past infancy. This is the medical baseline.
What a Deeper Look Adds
Once a child is past infancy and eating solid foods, most measurable health gains from breastfeeding are more modest than in early months — particularly for well-nourished children in settings with clean water and safe formula.² The phrase “mutually desired” matters enormously. A mother who is exhausted, touched out, or resentful is not in a situation medicine can fix — that is a question of family functioning and personal values.
A note on required scenarios:
Can’t breastfeed or finds it painful: Pain beyond the first few weeks is not required. Mastitis, poor latch, or low supply are common medical issues; a lactation consultant can help, but stopping is a valid choice.
Pumping: A demanding but genuine middle path. Widely used by working mothers.
Exhaustion and sleep: Nighttime nursing can feed both baby and sleep deprivation. See Issue V.
Pressure and criticism: None of those people are responsible for your child’s wellbeing. You are.
Early formula transition: Modern formula is safe, regulated, and nutritionally adequate. No legitimate guilt is owed.
Continuing at 2+; family calls it “weird”: The AAP supports this. “Weird” is a social judgment, not a medical one.
Nursing to sleep; feeling trapped: A sleep-association issue (see Issue V), not a character flaw. Addressable through gradual weaning.
Stopping and child’s behavior worsens temporarily: Common and normal. Temporary distress is not evidence of harm.
What changed over time: Formula was aggressively marketed in the mid-20th century as modern and superior; breastfeeding declined sharply in the 1950s–1970s. Public health evidence — especially in developing countries — triggered a reversal, including the WHO’s 1981 International Code of Marketing of Breast-milk Substitutes. The AAP updated its guidance from one year to two years in 2022.³
What’s Controversial / Unsettled
Whether extended breastfeeding (past 18–24 months) improves cognitive outcomes in well-nourished children is unsettled — some studies show modest gains; others show negligible effects once socioeconomic factors are controlled.
Whether nursing “spoils” a child is a folk belief with no credible evidence.
Evidence snapshot: High confidence for first 6 months; Moderate confidence for 6–24 months; Low confidence beyond 24 months for most health outcomes.
Bias Watch
Lactation consultants are professionally rewarded for promoting breastfeeding and may understate difficulty or pain.
Formula companies have decades of documented marketing bias.
Pediatricians broadly support extended nursing but may lack nuance about the mother’s experience.
Online communities — both pro-formula and pro-extended nursing — treat personal anecdotes as universal truths.
Practical Takeaways
Breastfeed if you can and want to. Stop if you need to. Both choices are legitimate.
The how long question is less important than the family’s overall functioning.
If nursing feels like a trap, it may have become one. Permission to wean is not a medical failure.
Six Pillars connection: Responsibility — for your child’s health and your own — and Respect for your own physical and emotional limits are both ethical values. Taking care of yourself is not selfishness; it is a precondition for good parenting.
II. Values and Character Formation
“Not every normal behavior is acceptable behavior. Preschoolers need both understanding and moral direction.”
The Parent Worry
Many parents today are uncomfortable about moral instruction. They don’t want to “impose” values. They worry that correcting a child’s behavior will damage self-esteem or create shame. Some have absorbed the idea that a child’s job is to express themselves, and the parent’s job is to support that expression. The result, in some homes, can be a kind of values vacuum — where children receive emotional support but very little moral direction.
What’s Normal at This Age
Preschoolers are beginning to understand right from wrong — but their understanding runs ahead of their impulse control. They know a rule before they can reliably follow it. Not every impulsive act is a sign of bad character; it may simply reflect an immature nervous system. The goal is to teach, not to shame.
What Mainstream Pediatric Guidance Emphasizes
Pediatricians and child development professionals broadly support the teaching of prosocial values — sharing, fairness, kindness — through modeling, positive reinforcement, and age-appropriate consequences. There is broad agreement that early childhood is an important period for prosocial learning, attachment, habit formation, and self-control.
What Matters Long-Term
Michael Josephson, founder of the Josephson Institute of Ethics and the CHARACTER COUNTS! program, spent decades arguing that moral literacy — the ability to recognize right from wrong and act accordingly — is a teachable skill.⁴ Values are core beliefs that drive conduct. They are not innate. They are formed — through what parents model, what they enforce, what they overlook.
His Six Pillars of Character — Trustworthiness, Respect, Responsibility, Fairness, Caring, and Citizenship — were identified in 1992 by a nonpartisan panel of youth development experts as ethical values that transcend cultural and religious differences.⁵ The TAME method — Teach, Advocate, Model, Enforce — is CHARACTER COUNTS!’s practical framework:
Teach = name the rule or value clearly.
Advocate = explain why it matters.
Model = do it yourself, visibly.
Enforce = respond when the rule is broken.
The principle: what you allow, you encourage.
Healthy guilt says, “I did something wrong and should repair it.” Shame says, “I am bad” — and shame makes change harder. The goal is an internal conscience, not obedience built on fear.
Large-scale surveys by the Josephson Institute across the 1990s through 2010s consistently found significant youth ethical concerns — including rates of admitted cheating and dishonesty high enough to prompt calls for renewed focus on character education in schools and homes.⁶
What changed over time: Moral instruction was once direct and explicit — children were told clearly what was right and wrong, often in religious frameworks. The late 20th century saw a shift toward values neutrality, driven by cultural pluralism, therapeutic culture, and fear of shaming. Values neutrality is itself a value system. Choosing not to judge is a judgment.
Reasonable families will differ about why honesty, fairness, or kindness matter — whether those reasons are religious, philosophical, communitarian, or something else. Parents committed to gentle parenting, progressive education, or therapeutic frameworks often share the same prosocial goals as parents who favor more direct moral instruction; the genuine disagreement is usually about method, tone, and authority, not whether children should develop honesty, empathy, and fairness.
What’s Controversial / Unsettled
Whether moral clarity creates authoritarianism is value-driven controversy. The evidence supports moral instruction; the method matters.
Religious and secular families differ in frameworks but share many core values.
Evidence snapshot: High confidence that warm, consistent, values-modeled parenting shapes long-term prosocial behavior; Moderate confidence on specific methods of moral instruction; Unsettled on the best way to resolve disagreements between cultural/religious and secular approaches.
Bias Watch
Therapeutic culture can overweight emotional safety and underweight moral direction.
Religious traditions may overemphasize sin and underweight developmental readiness.
“Gentle parenting” ideology at its weakest inadvertently models values neutrality — but at its best integrates emotional attunement with clear values. The difference matters.
Traditional authority frameworks can prioritize obedience over internalization.
Three Real-Life Scenarios
“My child took a toy and denied it.” It is developmentally normal — and it is also wrong. Both things are true. Say clearly: “Taking something that isn’t yours is not okay. We tell the truth.” Then address it calmly.
“My child mocked another child.” Correction without shame: “What you said hurt him. That’s not how we treat people. Caring about how others feel matters in our family.”
“I promised a consequence and backed down.” You may have taught your child that your rules are flexible. Trustworthiness — one of the Six Pillars — includes parental reliability. Follow through, even when inconvenient.
Practical Takeaways
Teach values by name. “That was unfair to your sister” is better than “Stop it.”
Model the behavior you want. Children absorb what they observe more than what they hear.
Enforce consistently. Inconsistency is not kindness — it is confusion.
III. Big Feelings: Tantrums, Meltdowns, and Emotional Regulation
The Parent Worry
A toddler screaming in the grocery store produces a particular kind of parental paralysis — equal parts embarrassment, exhaustion, and uncertainty. Modern parenting culture loads parents with contradictory messages: “Never ignore a feeling” but also “Don’t give in to manipulation.” The result is parents who freeze.
What’s Normal at This Age
Tantrums peak between ages 18 months and 3 years. The child’s prefrontal cortex — the brain region managing impulse control — is developmentally immature during the preschool years.⁷ This is biology, not bad parenting. A 3-year-old who hits when frustrated does not have an “aggressive personality.” They have an immature nervous system and an insufficient vocabulary for frustration.
What Mainstream Pediatric Guidance Emphasizes
Mainstream pediatric and public-health guidance teaches parent skills: calm limit-setting, consistent routines, modeling, and emotion labeling. These are now considered core competencies of early childhood caregiving, not just therapeutic tools.
What Changed Over Time
Strict obedience norms once dominated (“Stop crying or I’ll give you something to cry about”). Behaviorism introduced time-outs as a neutral consequence. The 1990s and 2000s brought emotion coaching — the insight that naming and validating feelings can reduce meltdowns. The current “gentle parenting” movement extended this into something more prescriptive: always validate, never punish. That goes further than the evidence supports.
Evidence snapshot: Moderate-to-high confidence that emotion coaching helps; Low-to-moderate confidence that any single approach is universally superior.
What’s Controversial / Unsettled
“Never punish negative emotions” is sound advice. “Never use consequences for behavior” is not the same claim — and is unsettled and contested.
Whether emotions must always be validated before limits are set is a reasonable principle — but validating a screaming child who is throwing objects can sometimes reinforce the behavior.
Bias Watch
Gentle parenting content creators on social media often show curated moments not representative of how consistently their methods work.
Behaviorists may underweight emotional experience. Emotion coaches may underweight behavioral accountability.
Three Real-Life Scenarios
Grocery store meltdown. Don’t give in to stop the screaming — that teaches screaming works. Remove the child calmly if possible. Name the feeling briefly: “You’re frustrated.” Then hold the limit. Most tantrums will end once the reinforcer is removed.
Three-year-old hits when frustrated. Address the behavior immediately and firmly: “Hitting hurts. We don’t hit.” Then — once calm — build vocabulary: “What can you do when you feel that way?”
Explosive at home, calm at school. This pattern is fairly common and can reflect that home feels safe enough to release tension. That said, context matters: if the behavior is frequent, severe, or accompanied by other concerns, it may also reflect masking, fatigue, overstimulation, or a developmental issue worth exploring.
Practical Takeaways
Feelings are valid. Behaviors have limits. These two things coexist.
Name feelings but don’t negotiate with meltdowns in progress.
After the storm passes, teach — don’t punish retrospectively.
Six Pillars connection: The long-term goal here is self-control — one of the core capacities underpinning every Pillar — and Caring about how our behavior affects others.
IV. Discipline and Consequences: Authority Without Cruelty
The Parent Worry
Parents fear two extremes: being too harsh (damaging the child) or too soft (raising a child who never learns limits). The pendulum in professional culture has swung hard toward “positive parenting,” leaving many parents unsure whether any consequence is appropriate.
What’s Normal at This Age
Children aged 2–5 can understand simple cause-and-effect. They cannot process lengthy lectures during or immediately after conflict. For a 2-year-old, consequences should be immediate and brief. A 4–5-year-old can handle short discussion, simple restitution, and occasionally a slightly delayed consequence.
What Mainstream Pediatric Guidance Emphasizes
The AAP and major pediatric organizations oppose corporal punishment and support positive discipline — clear expectations, consistent follow-through, and explanations that connect behavior to values, not just rules.⁸
What Changed Over Time
Corporal punishment was once standard — supported by law, culture, and some religious traditions. Research beginning in the 1990s documented its harms: increased aggression, poorer mental health outcomes, damaged parent-child trust.⁸ Evidence snapshot: High confidence that harsh physical punishment causes harm; Moderate confidence on optimal alternative methods.
What’s Controversial / Unsettled
Time-out is contested in popular culture — some online claims call it “harmful.” Research does not support that label when time-out is used correctly: brief, calm, connected to the behavior, followed by re-engagement. Note: Children with trauma histories, sensory differences, or certain developmental conditions may need adapted or alternative approaches; a brief time-out may not be the right tool for every child.
The distinction between compliance and internalization matters. A child who obeys only because of punishment has not internalized values. The goal is internalization.
Bias Watch
Therapeutic culture has sometimes conflated appropriate correction with harm.
Traditional religious frameworks sometimes use obedience as the primary value, underweighting understanding.
Three Real-Life Scenarios
“Stop throwing the toys” — threat not followed through. You may have trained your child that your words don’t matter. Pick fewer battles. But when you set a limit, hold it.
Preschooler lies about breaking something. Lying at 3–4 is developmentally common but not morally inconsequential. “I need to be able to trust what you tell me. That’s important.” Don’t over-punish. Do take it seriously.
Child hits sibling; time-out vs. restitution. Both can work. Time-out addresses the behavior. Restitution addresses the relationship: “You hurt your sister. What can you do to make it better?” Combining them is often most effective.
Practical Takeaways
Authority is not cruelty. Children need structure and limits.
Be firm, calm, and brief. Long lectures don’t work with preschoolers.
The goal of discipline is teaching — not punishment for its own sake.
Six Pillars connection: Effective discipline teaches Responsibility, Fairness, and Trustworthiness — in the parent as much as the child. Follow-through is itself a moral act.
V. Sleep: The Invisible Driver
The Parent Worry
Sleep deprivation is one of the top reasons parents seek help. When a child won’t sleep, nothing else works well — not patience, not consistency, not even good values. A parent who is chronically exhausted cannot parent intentionally.
What’s Normal at This Age
For infants, safety guidance dominates — the AAP advises against bed-sharing due to SIDS risk.⁹ For toddlers and preschoolers, the main issues shift to habits, routines, and parental consistency. Preschoolers (ages 3–5) need 10–13 hours of sleep per day, including naps.¹⁰ Sleep deprivation in young children drives behavior problems, learning difficulties, and emotional dysregulation — sometimes mimicking ADHD. Parental sleep deprivation drives inconsistency, anger, and despair.
What Mainstream Pediatric Guidance Emphasizes
Consistent bedtime routines — a regular sequence of calming activities before bed — are the most evidence-supported intervention, recommended across virtually all major pediatric and sleep medicine organizations.
What Changed Over Time
Ferber-style and other graduated sleep-training methods were highly influential for decades. Online culture has heavily stigmatized sleep training, sometimes claiming it causes lasting harm. The evidence does not support the harm claim. Evidence snapshot: High confidence that sleep deprivation harms children and parents; Moderate confidence on best methods; Low confidence on long-term harms of sleep training used appropriately.
It is also worth acknowledging that cultural norms, housing arrangements, work schedules, and access to childcare significantly shape how sleep is structured in different families. What works in one household may not be possible in another. (
What’s Controversial / Unsettled
Claims that sleep training causes “attachment damage” are widely circulated online but lack strong evidence. Multiple studies have found no lasting psychological harm from graduated sleep training in healthy children.
Co-sleeping past the infant window is genuinely values-driven, not purely medical.
Bias Watch
Anti-sleep-training communities online amplify rare distress cases as universal outcomes.
“Attachment parenting” ideology can make parents feel that any sleep separation is abandonment.
Three Real-Life Scenarios
Child wakes nightly and demands parent presence. Consistency is the active ingredient. A graduated approach — gradually reducing your presence over nights — is backed by moderate evidence and is not cruel.
Naps at daycare, awake until 10 p.m. Work with the daycare on nap timing. Consistent routines — bath, book, bed — are the most evidence-supported intervention.
Child refuses bedtime and parent negotiates for an hour. Reduce the nightly negotiation and move toward a firm, predictable routine.
Practical Takeaways
Prioritize sleep as a non-negotiable health need — yours and theirs.
Consistent routines beat any single technique.
Sleep training is not cruelty. Chronic sleep deprivation has documented harms.
Six Pillars connection: Teaching a child to self-settle builds Responsibility and emotional self-control — capacities that extend far beyond bedtime.
VI. Bottles, Food, Picky Eating, and Control
The Parent Worry
Food becomes a battleground in most families with toddlers and preschoolers. Parents fear malnutrition. They fear eating disorders. They’ve read about “clean your plate” causing obesity and “pressure to eat” causing disordered eating — and they’re not sure what’s left.
What’s Normal at This Age
Picky eating is near-universal in ages 2–5, affecting a large proportion of preschool-aged children. It is largely driven by food neophobia — an evolutionarily adaptive caution toward unfamiliar foods. Many children broaden their diets over time, especially without coercive pressure.
Bottles: Prolonged bottle use beyond 12–18 months is associated with increased cavity risk and potential speech effects. Transition to a cup by 12 months is standard guidance, though many toddlers resist.
Red flags: weight loss, choking or gagging at meals, severe sensory restriction, nutritional deficiency, or meals that consistently turn into panic.
What changed over time: “Clean your plate” was the postwar cultural norm. Obesity concerns in the 1980s–90s shifted guidance toward responsiveness. Ellyn Satter’s Division of Responsibility model — parent decides what and when; child decides how much — became the dominant professional framework and has moderate research support.
What’s Controversial / Unsettled
Sugar causes hyperactivity is a persistent myth. Multiple double-blind controlled studies find no effect.¹¹
Whether “pressure to eat” causes eating disorders is moderately supported — chronic pressure is associated with worse outcomes.
Bias Watch
Dietitians may overemphasize variety; pediatricians may understate feeding difficulties.
“Clean eating” social media culture pathologizes normal picky eating.
Three Real-Life Scenarios
Child eats only beige foods. Textbook food neophobia. Offer variety without pressure.
Child tantrums for snacks; parent gives in. Structure snack times. Do not negotiate with a tantrum.
“One more bite” battles every night. Stop. Offer what you’ve decided. Remove the plate calmly when the meal ends.
Practical Takeaways
Picky eating is common and often self-resolving.
Structure when and what is offered; don’t control how much is eaten.
Consult a professional if a child eats an extremely narrow range of foods, is losing weight, or gags consistently.
Six Pillars connection: Mealtime teaches Respect — for food, for the family’s effort, and for others at the table.
VII. Pacifiers and Thumb-Sucking
The Parent Worry
Parents are told pacifiers prevent SIDS, then told they cause dental problems, then told they delay speech, then told thumb-sucking is worse. It is genuinely confusing.
What’s Normal at This Age
Pacifiers in infancy carry a well-supported association with reduced SIDS risk — likely because they help maintain arousal during sleep. This benefit is specific to infancy.¹² After the first year, the medical calculus changes.
Mainstream pediatric and dental guidance treats occasional soothing use in toddlers as manageable, but persistent daytime use after age 2–3 as a reason to begin weaning. Continued pacifier use past approximately age 3 is associated with dental changes — including open bite, protruding front teeth, and narrowed palate, per guidance from the American Academy of Pediatric Dentistry.¹³ Speech effects from pacifiers are mixed in evidence: all-day use reduces opportunities for vocalization and oral motor practice, but professional speech-language pathologist consensus does not support the claim that pacifiers directly cause speech delays.¹⁴
What Changed Over Time
Pacifiers moved from folk remedy to medical recommendation (SIDS prevention) to clinical concern (dental, speech) as evidence accumulated over decades.
What’s Controversial / Unsettled
“Pacifiers ruin attachment” is a folk claim without credible research support.
The SIDS benefit is specific to infancy — do not generalize it to justify continued use at age 3+.
Thumb-sucking is harder to eliminate and carries similar dental concerns past age 4.
Bias Watch
Dentists may emphasize cessation urgency beyond what some developmental research supports.
Parenting forums often normalize extended pacifier use past ages that concern pediatric dentists.
Three Real-Life Scenarios
Two-year-old requires pacifier or blanket. Normal transitional object use. Begin limiting to sleep times.
Three-year-old uses pacifier all day; daycare complains. Limit use to sleep and very distressed moments only. Have a plan to wean by age 3.
Four-year-old sucks thumb; parent fears braces. Concern is legitimate after age 4. Gentle redirection and positive incentives work better than shaming.
Practical Takeaways
Pacifiers are a net benefit in infancy. They become a net concern by age 3.
Wean pacifier use between ages 2 and 3 — gradually, kindly, but intentionally.
VIII. Screens and the Digital Ecosystem
“The main risk is not just the screen itself — it’s what the screen replaces: sleep, conversation, boredom, play, and the slow work of learning to tolerate frustration.”
The Parent Worry
Parents are bombarded with warnings: screens cause autism; screens cause ADHD; one more hour and your child’s brain is damaged. At the same time, they use screens to survive — to cook dinner, manage a meltdown, survive a long flight.
What’s Normal at This Age
AAP guidance discourages screen use before 18 months except video chatting, and emphasizes quality, context, and family media habits over rigid minute-counting for ages 2–5. For children 2–5, approximately one hour daily of high-quality programming, with co-viewing where possible, reflects the current professional standard.¹⁵ Avoid treating routine screen use before 18 months as a norm even if occasional exceptions occur.
Emerging research links excessive screen time in preschoolers to associations with neurodevelopmental outcomes, with parental co-engagement identified as a key mitigating factor.¹⁶ (Source language softened from “found” to “links … to associations with” to better reflect study design limitations.)
The main risks are not just the screen itself but what it displaces — sleep, conversation, outdoor play, boredom, and the slow practice of tolerating frustration.
What Mainstream Pediatric Guidance Emphasizes
The AAP’s current framing emphasizes a family media plan over a single universal time limit. What children watch, whether parents co-view and discuss content, and whether screens displace other essential activities matter as much as total minutes.
What Changed Over Time
1990s parenting focused on TV limits. Smartphones and tablets changed the landscape entirely — passive TV watching became interactive, personalized, algorithmically designed media. Many apps use variable-reward mechanisms to capture and hold attention.
What’s Controversial / Unsettled
Screens cause autism or ADHD: Not supported by evidence. Association studies suffer from severe confounding. Evidence: Low confidence — likely false.
“All educational apps are good”: Often marketing, not research. Many apps labeled “educational” have no peer-reviewed evidence of benefit.
Bias Watch
App developers and content companies have profound financial incentives to claim educational benefit.
Screen panic creates guilt disproportionate to evidence of harm.
Parent phone use is underemphasized in most professional guidance. Children model what they observe.
Three Real-Life Scenarios
Videos used to calm tantrums; child now demands screens to regulate feelings. This is a learned behavior — learnable means changeable. Replace gradually with a comfort object, a parent’s presence, or a different routine.
“Educational” content watched for hours; child won’t engage in play. Free play is the developmental work of early childhood. Time away from screens isn’t punishment. It’s restoration.
Parent is on phone constantly. This is the most underacknowledged screen issue in preschool parenting. Divided attention is the lesson being taught.
Practical Takeaways
Avoid routine screen use before 18 months; treat exceptions as exceptions.
About one hour daily for ages 2–5, with co-viewing and discussion.
Watch what you offer and how you interact around it, not just how long.
Your own phone use is part of your child’s screen environment.
Six Pillars connection: Self-control, Caring (noticing others when screens pull us inward), and Citizenship all begin in the earliest habits children develop around attention.
IX. Developmental Milestones: “Is My Child on Track?”
The Parent Worry
Nothing produces parental anxiety faster than a checklist that suggests a child is “behind.” The 20-month-old who says few words. The 3-year-old who lines up toys and avoids eye contact. Parents spiral between “wait and see” and “what if I’m missing something?”
What’s Normal at This Age
Development is not a single line — it is a broad range with meaningful variation. Milestone checklists are screening tools, not diagnoses. A passed checklist can miss a real concern; a failed checklist can flag a child who later develops typically.
What Mainstream Pediatric Guidance Emphasizes
The AAP recommends developmental screening at 9, 18, and 24–30 months, with autism-specific screening at 18 and 24 months. These are routine, not alarm-triggered.
What Changed Over Time
For most of the 20th century, pediatricians and families operated under “wait and see.” Beginning in the 1990s, research demonstrated that early intervention substantially improves outcomes for children with speech delays, autism spectrum disorder, and developmental disabilities.¹⁷ The shift was driven by outcome data. Milestone checklists became mainstream tools of that evidence base.
Evidence snapshot: High confidence that early intervention improves outcomes; Moderate confidence on screening accuracy; Unsettled on specific diagnostic boundaries, especially for autism spectrum.
What’s Controversial / Unsettled
Over-labeling vs. under-diagnosing: Both are real risks. Rates of autism identification have risen sharply; CDC reporting moved from about 1 in 36 to about 1 in 31 in the most recent surveillance update (2025). Whether this reflects better detection, broader criteria, or genuine prevalence increase is scientifically contested.
Cultural differences: Some milestones — eye contact, pointing — are culturally variable. Screening tools were largely developed on middle-class Western children.
Bias Watch
“Boys talk late” is one of the more misleading and potentially costly folk beliefs in early development. Boys do talk slightly later on average — but meaningful absence of words or gestures, or loss of previously acquired language, in the second year is a clinical flag regardless of sex.
Diagnostic inflation is a legitimate concern — not every meltdown-prone 4-year-old has ADHD.
Daycare liability anxiety can push parents toward evaluation unnecessarily.
Four Real-Life Scenarios
One-year-old not crawling. Some children skip crawling. Absence of any purposeful movement or weight-bearing by 12 months warrants a conversation with your pediatrician.
20-month-old says only a few words; grandparents say “boys talk late.” Lack of meaningful words, gestures, or social communication by the latter part of the second year is a clinical flag. Early speech therapy is effective; the cost of acting early is minimal.
Three-year-old avoids peers, lines up toys; daycare is worried. Take it seriously. Request an evaluation. A concern raised by consistent observers who see many children is not hysteria.
Four-year-old melts down with any change in routine. Rigidity around routine is common in preschoolers and is not by itself diagnostic. But if it is frequent, severe, and accompanied by other concerns, evaluation is appropriate and low-risk.
Practical Takeaways
A screening flag is a prompt to look closer, not a diagnosis.
“Wait and see” has a real cost when delays are involved.
Trust teachers and daycare providers who raise specific, consistent behavioral concerns.
Six Pillars connection: Caring and Responsibility require acting when a child may need help. Getting an evaluation is not a failure — it is a loving, responsible act.
X. Toilet Training, Bodily Autonomy, and Shame
The Parent Worry
Toilet training is one of the most anxiety-producing milestones of early childhood — for parents, children, and daycare providers alike. Parents worry about starting too early, starting too late, creating shame, or being judged by other parents whose children trained at 18 months. Some feel subtle pressure from daycares that require training by age 3 for classroom placement.
What’s Normal at This Age
Most children are developmentally ready for toilet training between 18 and 36 months, with a wide variation that is normal and not a predictor of later functioning.¹⁸ Readiness — not a calendar date — is the appropriate trigger. Signs include awareness of bodily functions, ability to follow simple instructions, and interest in the process. Girls statistically train slightly earlier than boys, but individual variation is larger than gender differences.
What Mainstream Pediatric Guidance Emphasizes
The AAP and most pediatric guidance supports a child-led, readiness-based approach rather than a fixed age or rigid schedule. Pressure, punishment, or forced sitting are associated with power struggles, withholding behaviors, and prolonged training.¹⁹ Most children who begin training at 2 are not reliably trained before 3; most children are reliably trained by age 4 regardless of when training began. (Note: the claim that “most children who start at 2 are not trained before 3” reflects established pediatric observation.)
What a Deeper Look Adds
Toilet training sits at the intersection of development, power, and autonomy. A child who feels coerced may resist not because they “can’t” but because they “won’t” — which is developmentally appropriate self-assertion, not defiance. The goal is to make the child feel capable and proud of mastering a skill — not ashamed of accidents or confused by unpredictable responses.
What changed over time: Early 20th-century approaches emphasized rigid training in the first year of life, driven by behaviorist principles and practical concerns (no disposable diapers). The later 20th century shifted toward child-readiness approaches, pioneered by pediatrician T. Berry Brazelton in the 1960s. The widespread adoption of disposable diapers extended the practical window. Today’s culture includes both the child-readiness model and a growing competitive parent culture around early training, amplified online.
What’s Controversial / Unsettled
“Three-day toilet training” methods are widely popular online. Evidence for their superiority over gradual readiness-based approaches is limited and not well-controlled.
Whether daycare pressure to train by age 3 is appropriate depends on the child’s developmental readiness — and is a legitimate stakeholder tension worth naming directly with caregivers.
Cross-cultural variation is significant; many cultures train earlier without apparent harm; the research base is primarily Western.
Bias Watch
Competitive parent culture treats early training as a developmental achievement rather than a readiness milestone.
Daycare policies create institutional pressure that may not reflect individual developmental needs.
Online “training experts” often promote proprietary methods without peer-reviewed support.
Three Real-Life Scenarios
Child seems ready at 20 months; family wants to begin. If the child shows genuine readiness signs, beginning is appropriate. Don’t rush to prove it’s possible; let the child’s pace drive it.
Three-year-old still having accidents; daycare is concerned. Have your pediatrician rule out medical causes. Use encouragement, not shame. Many children need until 3½ or later.
Child was trained, then regressed. Regression is common after a major change — new sibling, move, illness. Treat it matter-of-factly. Shame about regression makes it worse and last longer.
Practical Takeaways
Wait for readiness. Starting before readiness is ready rarely shortens the overall process.
Avoid shame — accidents are not moral failures.
If training is not progressing by age 4, consult your pediatrician to rule out medical or developmental causes.
Six Pillars connection: Respect for the child’s developing autonomy, Caring in how we respond to accidents, and Responsibility in building a new self-care skill are all in play. How we handle accidents teaches children how failure should feel — like something to correct, not something to be ashamed of.
An Anchoring Note
“You do not need perfection. You need intention — and attention.”
You don’t need to be perfect. But you do need to be intentional. Most ordinary parenting decisions are recoverable — the research consistently shows that what matters most is not any single practice but the presence of a warm, consistent, values-driven parent. That said, a few areas genuinely deserve prompt attention: sleep safety in infancy, developmental delays, harsh or punitive discipline, and persistent medical concerns that are not addressed. Relax about the rest. You are almost certainly doing better than the internet makes you feel.
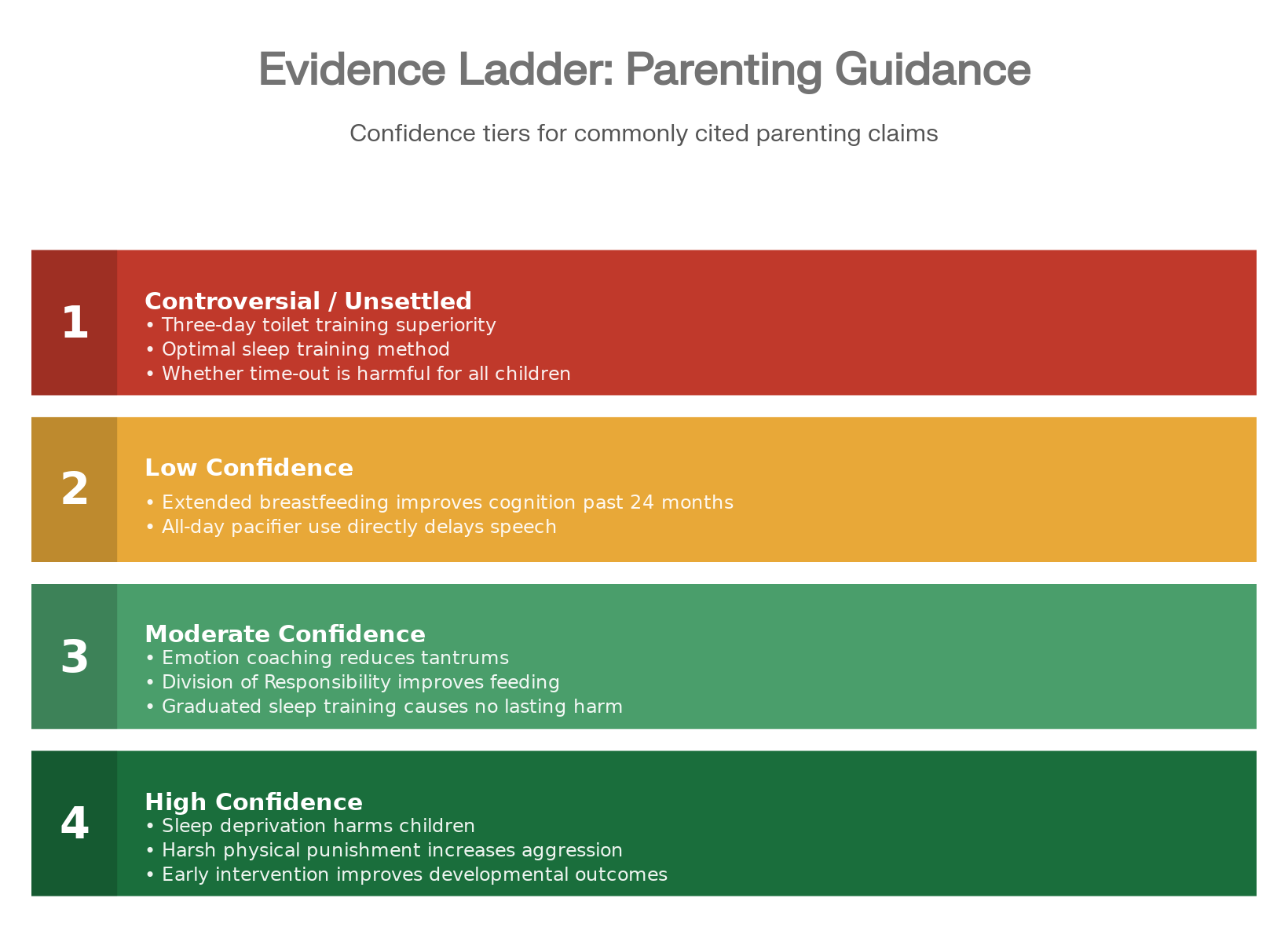
The Evidence Ladder — What We Know and How Confident We Are
Reliable Resources
This section is curated, not exhaustive. Each resource is assessed for quality, bias, and fit.
Books
The Whole-Brain Child by Daniel J. Siegel and Tina Payne Bryson (2011). Best for: Understanding why toddlers and preschoolers react as they do; connecting neuroscience to practical strategy. Blind spot: Leans heavily on therapeutic culture; limited moral formation content. Lean: Psychological/therapeutic.
No-Drama Discipline by Daniel J. Siegel and Tina Payne Bryson (2014). Best for: Brain-science-based approaches to behavior emphasizing connection before correction. Blind spot: Can underemphasize that some behaviors require immediate consequences. Lean: Psychological/therapeutic.
Raising Good Humans by Hunter Clarke-Fields (2019). Best for: Integrating mindfulness and values into everyday parenting. Blind spot: Assumes significant parental capacity for self-regulation; may feel idealistic for exhausted or single parents. Lean: Secular/mindfulness-oriented.
CHARACTER COUNTS! curriculum materials from the Josephson Institute of Ethics. Freely available at josephsoninstitute.org and charactercounts.org. Essential for parents focused on moral formation.
Touchpoints: Birth to Three by T. Berry Brazelton and Joshua Sparrow (2006). A developmental pediatrician’s guide to predictable developmental disruptions. Less ideological; grounded in clinical observation. Especially useful for toilet training, sleep, and feeding.
Caring for Your Baby and Young Child: Birth to Age 5 — American Academy of Pediatrics (7th ed., 2019). The standard pediatric reference. Comprehensive and evidence-based. Supplemented by current guidance at healthychildren.org.
ENDNOTES
American Academy of Pediatrics. “Breastfeeding and the Use of Human Milk.” Pediatrics, updated February 2026.
Eidelman, Arthur I., and Richard J. Schanler. “Breastfeeding and the Use of Human Milk.” Pediatrics 129, no. 3 (2012): e827–e841. [Updated per AAP 2022 policy.]
Feldman-Winter, Lori. “Breastfeeding: AAP Policy Explained.” HealthyChildren.org, May 16, 2024.
Josephson Institute of Ethics. “The Six Pillars of Character.” josephsoninstitute.org, updated 2025.
CHARACTER COUNTS! “Model Standards for Education.” Josephson Institute, January 2025.
Josephson Institute of Ethics. Youth ethics surveys, 1992–2012.
Diamond, Adele. “Executive Functions.” Annual Review of Psychology 64 (2013): 135–168. [Replaces the previously flagged Casey et al. 2008 adolescent brain citation; Diamond’s work is specific to preschool-age executive function and prefrontal cortex development.]
Gershoff, Elizabeth T. “Corporal Punishment by Parents and Associated Child Behaviors and Experiences.” Psychological Bulletin 128, no. 4 (2002): 539–579. See also AAP Policy Statement. “Effective Discipline to Raise Healthy Children.” Pediatrics 142, no. 6 (2018).
American Academy of Pediatrics. Safe Sleep Guidelines for Infants. Updated 2022. healthychildren.org.
American Academy of Sleep Medicine.
Wolraich, Mark L., et al. “The Effect of Sugar on Behavior or Cognition in Children.” JAMA 274, no. 20 (1995): 1617–1621.
Moon, Rachel Y. and AAP Task Force on Sudden Infant Death Syndrome. “SIDS and Other Sleep-Related Infant Deaths.” Pediatrics 138, no. 5 (2016).
American Academy of Pediatric Dentistry. Policy on Oral Habits.
American Speech-Language-Hearing Association (ASHA). Position on pacifiers and speech.
American Academy of Pediatrics. “Media and Children.” HealthyChildren.org.
PMC/NIH. “Screen Time and Neurodevelopment in Preschoolers.” January 12, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12146794/
Guralnick, Michael J. “Why Early Intervention Works.” Infants and Young Children 24, no. 1 (2011): 6–28.
Brazelton, T. Berry. “A Child-Oriented Approach to Toilet Training.” Pediatrics 29 (1962): 121–128. See also: Stadtler, Ann C., et al. “Perceptions of Readiness for Toilet Training.” Pediatric Nursing 25, no. 4 (1999).
Taubman, Bruce. “Toilet Training and Toileting Refusal for Stool Only.” Pediatrics 99, no. 1 (1997): 54–58.
https://josephsoninstitute.org/wp-content/uploads/2015/09/ji-logo.png00Michael Josephsonhttps://josephsoninstitute.org/wp-content/uploads/2015/09/ji-logo.pngMichael Josephson2026-04-06 16:01:162026-04-06 18:02:09PRACTICAL PARENTING YOUR PRE-SCHOOLER IN 2026: PERSPECTIVES, PROOF AND POSSIBLE ACTIONS
0replies
Leave a Reply
Want to join the discussion? Feel free to contribute!

Leave a Reply
Want to join the discussion?Feel free to contribute!